A great case yesterday had some anatomic features that I thought worth showing. This gentleman was a firefighter who had an accident at work and following this developed debilitating migraines. For privacy purposes we will call him Frank here. Frank is from Denver, and as such he had seen several doctors including Denver neurologists who had tried to manage his pain with medications including triptans, though unsuccessfully.
When Frank initially came to see me for an evaluation of his migraine headache pain, we performed our Targeted Injection Mapping using nerve blocks to figure out exactly which nerves were bothersome for him. Unfortunately for Frank, he had nerve irritation in the front and the back causing headache pain in the forehead behind his eyes, as well as in the back of his head in the occipital region. He chose to have surgery on the frontal nerves first, and so we released his supra-orbital, supra-trochlear, zygomaticotemporal, and auriculotemporal nerves in his first operation with great success. Frank had complete resolution of his frontal migraine headaches following this operation, and had now decided to pursue relief of his migraine headaches in the back.
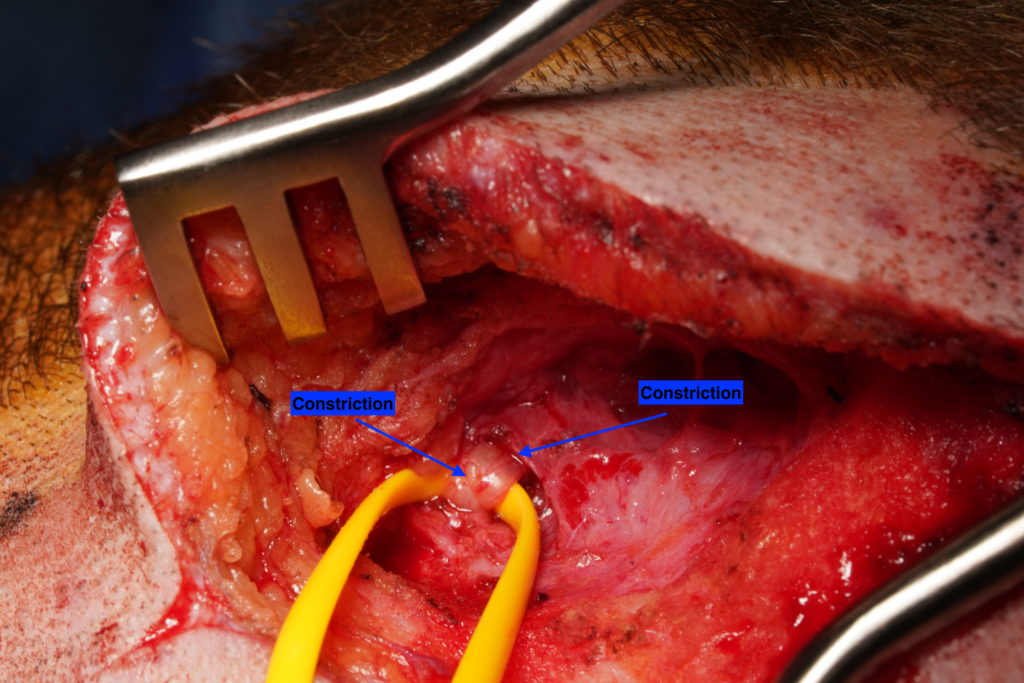
During Frank’s operation, I started work on the left side because this was the side on which Frank had the worst migraine pain. Here in the photo below, you can see the early exposure of the Greater Occipital Nerve coursing through the trapezius muscle, and immediately it is evident how this nerve had several areas of compression/constriction.
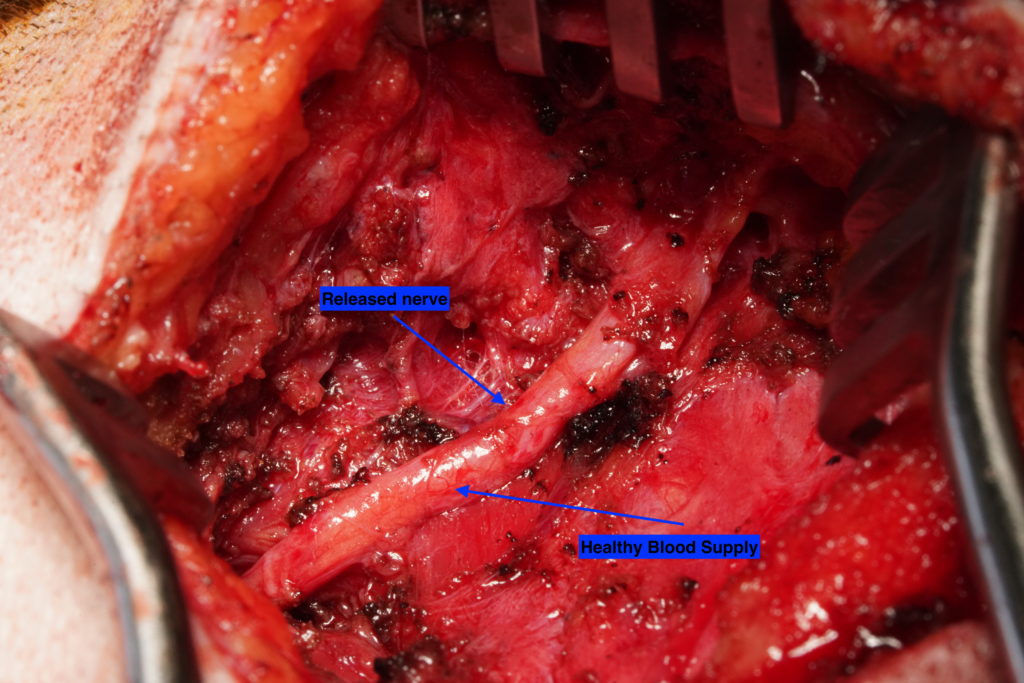
The nerve on this side ran quite deeply in the semispinalis muscle, a significant amount of dissection was required to release this nerve in a manner where it lay in a relaxed fashion without the repeated squeezing from the surrounding muscle by even the action of keeping Frank’s head erect. You might imagine that when stressed or active, such muscle commonly squeezed further on this nerve, creating irritation that sent signals of pain to the brain and caused his headache pain. In the photo below, you can see how the released nerve is no longer constricted, and additionally the nerve can be seen to be plump and healthy, with intact blood vessels in what is called the peri-nuerium, or coating of the nerves. These blood vessels, when constricted from the surrounding tissue, can cause the nerve to not get enough blood and oxygen, and so this perpetuates the nerve irritation and pain syndrome. Now that the nerve is free and relaxed, the blood supply is healthy and can help the nerve to function normally.
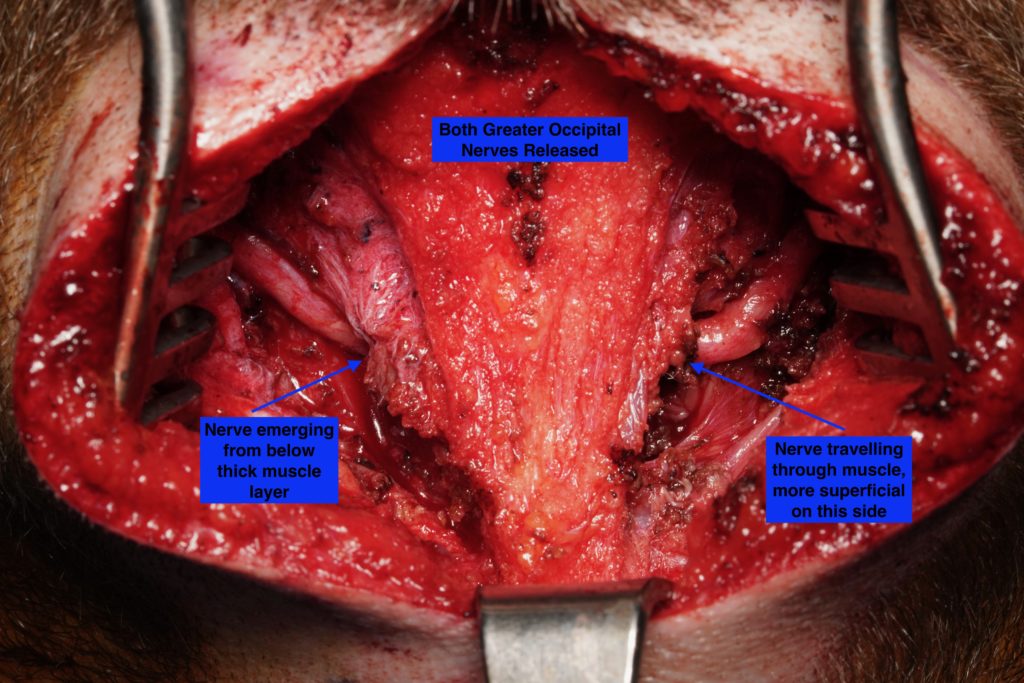
The photo below is interesting because it shows the difference in the anatomy from the left side to the right side. On the right side the nerve was found to be much more superficial. In the photo, the layer of muscle toward the center fo the photo can be seen to be thinner, and you can see how the nerve emerges from less deeply on this side. Though both nerves originate at the same level from the nerve roots near the spine, the nerve one either side can take different paths. The one on Frank’s left travelled longer through tight muscle, while the Greater Occipital Nerve on the right was less encased in muscle and not surprisingly, less symptomatic and causing less migraine pain.
A great case all in all, and as Frank recovers from his outpatient surgery I’m looking forward to a response similar to his frontal nerve release where his migraine pain is greatly relieved and improved. If you are having ongoing difficulty with migraine pain in the front or back or both sides of your head and neck, please call our Migraine Surgery Specialty Center at 805-969-9004 and I will be happy to discuss your particular case with you in an effort to help you find a permanent migraine cure.
